
Muscles Don't Work Alone. The Role of Fascia and Muscular Connections in Effective Massage
1. A Brief on the Basics: Bones, Muscles, and Fascia
Bones (Skeleton): Imagine them as the sturdy frame of our body. They provide support, protect internal organs, and serve as “anchors” to which muscles attach. Movement is only possible because muscles can pull on bones.
Muscles: These are our “engines.” Their main ability is to contract and relax. When a muscle contracts, it pulls on a bone via tendons. We will mainly talk about skeletal muscles—the ones you work with during a massage.
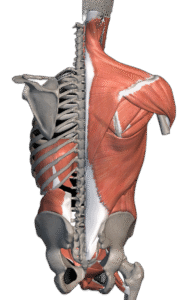
And Then There’s Fascia! Picture a thin but strong spiderweb or an elastic “bodysuit” that permeates our entire body. This is fascia—a special type of connective tissue. It envelops every muscle, every muscle fiber, entire muscle groups, organs—literally everything!
What is it for? Fascia provides support and shape, helps muscles glide over each other during movement, but most importantly for us—it connects all parts of the body into a single, continuous network and can transmit tension.
How does movement happen? Muscles often work in pairs or groups (agonists/antagonists). When one contracts, the other must relax. Understanding this balance and the role of fascia in this process is crucial.
2. Main Muscles You Often Work With (by Zone)
Here we will list some key muscles, their main functions in simple terms, and where to generally find them.
A. Back and Posterior Neck:
Trapezius muscle (“Traps”): A large, cloak-like muscle from the base of the skull to the middle of the back.
Upper part: Lifts the shoulders (“shrugging”), involved in tilting and turning the head. Often tense due to stress and sitting at a computer.
Middle part: Pulls the shoulder blades together.
Lower part: Depresses the shoulder blades.
Rhomboid muscles (Major and Minor): Located under the trapezius, between the spine and the shoulder blades. Function: Pull the shoulder blades toward the spine. Often weakened and stretched in people with rounded shoulders.
Latissimus dorsi (“Lats”): The largest muscle of the back, running from the armpit down to the pelvis and spine. Function: Pulls the arm down and back (as in rowing), brings the arm toward the torso.
Erector spinae muscle: This is not a single muscle, but a group of long muscles along the entire spine. Function: Extend the back (straighten us up), maintain posture. Often overloaded with a weak core or improper lifting of heavy objects.
Quadratus lumborum (QL): A deep muscle in the lower back, from the pelvis to the ribs and lumbar vertebrae. Function: Tilts the torso to the side, helps stabilize the lower back. Often associated with lower back pain.
B. Anterior Neck and Shoulders:
Sternocleidomastoid muscle (SCM): A prominent band on the side of the neck, running from the temple area behind the ear to the clavicle and sternum. Function: Tilts the head to its own side, turns it to the opposite side; when both contract, it flexes the head forward. Often shortened in cases of “tech neck.”
Scalene muscles: A group of three muscles deeper than the SCM, on the side of the neck. Function: Help tilt the neck, lift the upper ribs during breathing. Tension can cause discomfort that radiates down the arm.
Deltoid muscle (“Delts”): Forms the rounded contour of the shoulder. Function: The main muscle for abducting the arm (lifting it to the side). The anterior part helps lift the arm forward, the posterior part helps move it backward.
Rotator cuff muscles: A group of 4 deep muscles around the shoulder joint (supraspinatus, infraspinatus, teres minor, subscapularis). Function: Stabilize the shoulder joint, rotate the shoulder internally and externally. A frequent source of shoulder pain.
C. Chest and Abdomen:
Pectoralis major (“Pecs”): A fan-shaped muscle on the front of the chest wall. Function: Brings the arm toward the torso, rotates it inward (as in hugging). Often shortened in people with rounded shoulders.
Pectoralis minor: Lies underneath the pectoralis major. Function: Pulls the shoulder blade forward and down. Its tension greatly affects shoulder position.
Rectus abdominis (“Abs”): The “six-pack” muscles. Runs from the ribs to the pubic bone. Function: Flexes the torso forward, supports internal organs.
Oblique muscles (Internal and External): On the sides of the rectus abdominis. Function: Help flex the torso, rotate it, and bend it sideways.
D. Arms:
Biceps brachii (“Biceps”): On the front surface of the upper arm bone. Function: Flexes the arm at the elbow, helps turn the forearm palm-up (supination).
Triceps brachii (“Triceps”): On the back surface of the upper arm bone. Function: Extends the arm at the elbow.
Forearm muscles: Numerous muscles responsible for wrist and finger movements (flexion, extension). Often overloaded in those who work a lot with their hands (computer, tools).
E. Legs and Glutes:
Gluteus maximus: The largest muscle, forming the main bulk of the buttocks. Function: A powerful hip extensor (backward movement, as in standing up from a chair or walking uphill), rotates the thigh outward.
Gluteus medius and minimus: Located on the side and partially under the gluteus maximus. Function: Abduct the leg (move it to the side), stabilize the pelvis during walking. Their weakness is often linked to lower back or knee pain.
Quadriceps femoris (“Quads”): A large group of muscles on the front of the thigh. Function: The primary extensor of the lower leg (straightens the leg at the knee).
Hamstring muscles: A group of three muscles on the back of the thigh (biceps femoris, semitendinosus, semimembranosus). Function: Flex the leg at the knee, extend the hip. Often shortened, especially in people who sit a lot.
Gastrocnemius muscle: Forms the main bulk of the calf. Function: Plantarflexes the foot (as in standing on tiptoes), assists in knee flexion.
Soleus muscle: Lies underneath the gastrocnemius. Function: Also plantarflexes the foot.
3. The Most Interesting Part: Muscular and Fascial Chains and Interconnections
Now we get to the main point: muscles rarely get tense or sore in isolation. Our body creates compensations. If one muscle is weak or too tense (“tight”), other muscles and the fascia surrounding them react.
Why does this happen?
Muscular Compensation: Other muscles try to take over the job of a weak or overloaded muscle.
Fascial Tension: This is the key! Since fascia is a single network, tension in one place can be transmitted through it to completely different areas. Imagine pulling on the corner of a tablecloth—wrinkles will form across the entire surface. The same happens with fascia: if a muscle is tense, inflamed, or injured for a long time, the fascia around it can “thicken,” lose its elasticity, and “adhere” to adjacent layers. This creates a pull and tension that is sometimes felt far from the original problem.
Which muscle and fascial groups are particularly strongly connected?
“Upper Crossed Syndrome” (Neck – Shoulders – Upper Back – Chest):
What happens: During prolonged sitting, the upper trapezius, neck muscles (SCM, scalenes), and pectoral muscles often shorten, pulling the surrounding fascia with them. This pulls the shoulders forward. The rhomboids and middle/lower trapezius between the shoulder blades become stretched and weak, and their fascia is also under constant tension.
Consequences: Neck pain, headaches, a “dowager’s hump,” pain between the shoulder blades, rounded shoulders. The feeling of being “armored” in the shoulder girdle is often a combination of muscular and fascial tension.
What a massage therapist should do: Work not only on the muscles but also aim to affect the fascia (slow, deep, stretching techniques). Relax the anterior surface (pectorals, SCM) and tone the posterior surface (inter-scapular area).
“Lower Crossed Syndrome” (Low Back – Pelvis – Glutes – Hips):
What happens: The hip flexors (front) and erector spinae (back) are often shortened and tense, with their fascia thickened. The gluteal muscles and abdominals are weakened, and their fascial support is reduced.
Consequences: Lower back pain, an exaggerated lumbar curve, pelvic tilt.
What a massage therapist should do: Pay attention to stretching the front of the thigh and relaxing the lower back, including working with the fascia of these areas. Activate the gluteal and abdominal muscles.
Connection: Low Back – Glutes – Hamstrings (and their fascia):
What happens: Shortened hamstrings and their dense fascia pull the pelvis backward. Tension in the gluteal muscles and deep pelvic muscles (including their fascial sheaths) can compress nerves (like the sciatic nerve) and affect the lower back.
Consequences: Lower back pain, limited forward bend, pain in the buttock, pulling pain down the leg.
What a massage therapist should do: When there is lower back pain, always check the condition of the glutes and hamstrings, working on both the muscles and the fascia (e.g., myofascial release for these zones).
Connection: Calves – Foot – Knee – Thigh (Fascial Continuity):
What happens: Tense calf muscles and thickened fascia in the lower leg restrict foot movement. This tension is transmitted upward along fascial lines (e.g., the Superficial Back Line, which runs from the foot to the head!), affecting the knees, hips, and even the back.
Consequences: Pain in the Achilles tendon, foot, or knees.
What a massage therapist should do: Work on the calves and feet, remembering they are part of a larger system. Massaging the foot and calf can alleviate pain higher up the chain.
4. Why is this important for you as a massage therapist?
Understanding the role of fascia and muscular connections allows you to:
Find the true cause of pain: You will see not just the muscles, but also the tension in the fascial network.
Work more effectively: You will be able to influence the entire connected muscular and fascial chain. Many massage techniques (like deep tissue, myofascial release) are aimed specifically at releasing fascia.
Better understand the client’s body: You will feel not only muscular knots but also fascial “adhesions” and restrictions in gliding.
Give more precise recommendations: Advice on stretching and movement will take this interconnected system into account.
Conclusion
Our body is an incredibly intelligent system where everything is connected. Muscles and fascia rarely live their own lives; they constantly interact. By studying anatomy, muscle functions, and the role of fascia, you not only become more technically skilled but also begin to better “listen” to the client’s body. This is the key to not just temporarily relieving symptoms, but helping people find balance, freedom of movement, and a life without pain.